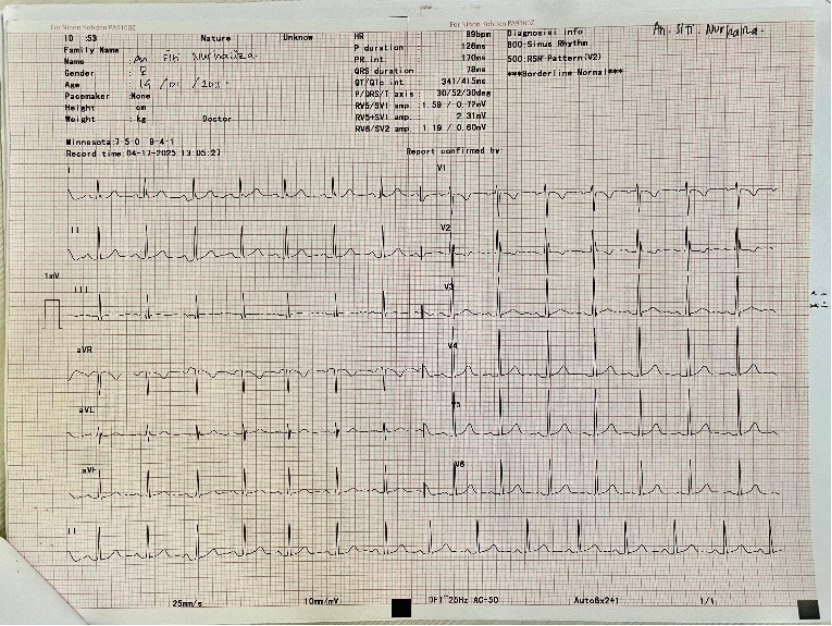
Rheumatic Chorea, also known as Sydenham Chorea, is a major neurological manifestation of acute rheumatic fever, an autoimmune complication following infection with Group A β-hemolytic streptococcus (GABHS). It remains common in low- and middle-income countries, where limited healthcare access may delay diagnosis and increase the risk of complications, particulary cardiac. We report a case of a 10-year-old girl from a remote area who presented with involuntary movements, joint pain, and a history of throat infection one month prior to symptom onset. Laboratory tests showed elevated erythrocyte sedimentation rate (ESR) and a positive Anti-streptolysin O (ASO) titer, indicating a recent streptococcal infection. Cardiac examination, including the electrocardiography (ECG), revealed no abnormalities. However, echocardiography, the gold standard for detecting subclinical carditis, was not performed due to lack of available resources. The patient was treated with haloperidol and trihexyphenidyl for chorea, penicillin G benzathine for eradication and prophylaxis of streotococcal infection, and aspirin for its anti-inflammatory effects. Clinical improvement was noted within one month of therapy. This case met the 2015 revised Jones criteria for moderate-risk populations, with major criteria including Sydenham chorea and polyarthralgia, and evidence of recent streptococcal infection (positive ASO). Absence of cardiac involvement may reflect early recognition and treatment, although echocardiography is required to exclude subclinical carditis. Symptomatic therapy and long-term antibiotic prophylaxis are crucial for preventing complications. Rheumatic Chorea can occur without cardiac involvement. Particularly in resource-limited remote areas, early diagnosis, adherence to Jones criteria, and secondary prophylaxis are essential to prevent long-term sequelae.
| Published in | American Journal of Pediatrics (Volume 11, Issue 4) |
| DOI | 10.11648/j.ajp.20251104.12 |
| Page(s) | 201-206 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Sydenham Chorea, Rheumatic Fever, Children, Without Cardiac Involvement, Case Report
Test | Result | Reference range |
|---|---|---|
Hemoglobin (g/dl) | 12,9 | 12-16 |
Hematocrit (%) | 40,6 | 38-47 |
Mean Corpuscular Volume (fl) | 87 | 80-100 |
White blood cells (cmm) | 8.300 | 4.000-10.000 |
Neutrophils (%) | 57 | 50-70 |
Lymphocytes (%) | 36 | 20-40 |
Platelet (cmm) | 240.000 | 150.000-450.000 |
Estimated sedimentation rate (mm/h) | 42 mm/I hour | 0-20 |
60 mm/II hour | ||
Anti-streptolysin O | (+) Positive | Negative |
SC | Sydenham Chorea |
RF | Rheumatic Fever |
ARF | Acute Rheumatic Fever |
ECG | Electrocardiogram |
ASO | Anti-Streptolysin O |
ESR | Erythocyte Sedimentation Rate |
GABHS | Group A β-Hemolytic Streptococcus |
CBGTC | Cortical-Basal Ganglia-Thalamo-Cortical |
GABA | Gamma Aminobutyric Acid |
IM | Intramuscular |
IVIg | Intravenous Immunoglobulin |
| [1] | Baizabal-Carvallo JF, Cardoso F. Chorea in children: etiology, diagnostic approach and management. J Neural Transm. 2020; 127(10): 1323-1342. |
| [2] | Deputy SR, Tilton AH. Treatment of disorders of tone and other considerations in pediatric movement disorders. Neurotherapeutics. 2020; 17(4): 1715. |
| [3] | Termsarasab P. Chorea. Continuum: Life Learning in Neurology. 2019; 25(4): 1001-1035. |
| [4] | Eyre M, et al. Treatments and outcomes among patients with Sydenham chorea: A Meta-Analysis. JAMA Netw Open. 2024; 7(4): 11-12. |
| [5] | Chowdhury MDS, Koziatek CA, Tristram D, et al. Acute Rheumatic Fever. Treasure Island (FL): StatPearls Publishing; 2025 Jan [cited 2025 Sep 28]. Available from: |
| [6] | Teixeira AL, et al. Sydenham’s chorea: from pathophysiology to therapeutics. Expert Rev Neurother. 2021; 21(8): 913-922. |
| [7] | Shahri HM, et al. Clinical findings of Sydenham chorea in pediatric patients: a single-center retrospective study. Ann Child Neurol. 2023; 31(3): 181-188. |
| [8] | Pons R. Sydenham’s chorea, PANDAS, and other post-streptococcal neurological disorders. In: Movement Disorder Emergencies. Cham: Springer; 2022. p. 255-270. |
| [9] | Patel NK, et al. Development and validation of RP-HPLC method for simultaneous estimation of haloperidol and trihexyphenidyl hydrochloride in tablet dosage form. Asian J Pharm Anal. 2022; 12(4): 253-7. |
| [10] | Beaton A, Carapetis J. The 2015 revision of the Jones criteria for the diagnosis of acute rheumatic fever: implications for practice in low-income and middle-income countries. Heart Asia. 2015; 7(2): 7-11. |
| [11] | Mohammad SS, Dale RC. Principles and approaches to the treatment of immune-mediated movement disorders. European Journal of Paediatric Neurology. 2018; 22(2): 292-300. |
| [12] | Vasconcelos LP, et al. Sydenham’s chorea: an update on pathophysiology, clinical features and management. Expert Opinion on Orphan Drugs. 2019; 7(11): 501-511. |
| [13] | Shadick NA, Karlson EW, Cook NR, Maher NE, Buring JE, Lee IM. Low-dose aspirin in the primary prevention of rheumatoid arthritis: the Women's Health Study. Arthritis Care Res (Hoboken). 2010; 62(4): 545-550. |
| [14] | Ralph AP, Noonan S, Boardman C, Halkon C, Currie BJ. Prescribing for people with acute rheumatic fever. PMC Home; 2017 Apr 3 [cited 2025 Sep 6]. Available from: |
| [15] | Farsana MK, Holla VV, Kamble N, Mahale RR, Arshad F, Pal PK, Yadav R. The burden of rheumatic chorea in the modern era: a case series from a tertiary health care center in South India. J Mov Disord. 2025; 18(3): 277-9. |
APA Style
Iwamony, V., Kristianti, N. G. H. (2025). Rheumatic Chorea Without Cardiac Involvement in a 10-Year-Old Girl from a Remote Area: Diagnostic and Management Challenges. American Journal of Pediatrics, 11(4), 201-206. https://doi.org/10.11648/j.ajp.20251104.12
ACS Style
Iwamony, V.; Kristianti, N. G. H. Rheumatic Chorea Without Cardiac Involvement in a 10-Year-Old Girl from a Remote Area: Diagnostic and Management Challenges. Am. J. Pediatr. 2025, 11(4), 201-206. doi: 10.11648/j.ajp.20251104.12
@article{10.11648/j.ajp.20251104.12,
author = {Violita Iwamony and Nyoman Gina Henny Kristianti},
title = {Rheumatic Chorea Without Cardiac Involvement in a 10-Year-Old Girl from a Remote Area: Diagnostic and Management Challenges
},
journal = {American Journal of Pediatrics},
volume = {11},
number = {4},
pages = {201-206},
doi = {10.11648/j.ajp.20251104.12},
url = {https://doi.org/10.11648/j.ajp.20251104.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20251104.12},
abstract = {Rheumatic Chorea, also known as Sydenham Chorea, is a major neurological manifestation of acute rheumatic fever, an autoimmune complication following infection with Group A β-hemolytic streptococcus (GABHS). It remains common in low- and middle-income countries, where limited healthcare access may delay diagnosis and increase the risk of complications, particulary cardiac. We report a case of a 10-year-old girl from a remote area who presented with involuntary movements, joint pain, and a history of throat infection one month prior to symptom onset. Laboratory tests showed elevated erythrocyte sedimentation rate (ESR) and a positive Anti-streptolysin O (ASO) titer, indicating a recent streptococcal infection. Cardiac examination, including the electrocardiography (ECG), revealed no abnormalities. However, echocardiography, the gold standard for detecting subclinical carditis, was not performed due to lack of available resources. The patient was treated with haloperidol and trihexyphenidyl for chorea, penicillin G benzathine for eradication and prophylaxis of streotococcal infection, and aspirin for its anti-inflammatory effects. Clinical improvement was noted within one month of therapy. This case met the 2015 revised Jones criteria for moderate-risk populations, with major criteria including Sydenham chorea and polyarthralgia, and evidence of recent streptococcal infection (positive ASO). Absence of cardiac involvement may reflect early recognition and treatment, although echocardiography is required to exclude subclinical carditis. Symptomatic therapy and long-term antibiotic prophylaxis are crucial for preventing complications. Rheumatic Chorea can occur without cardiac involvement. Particularly in resource-limited remote areas, early diagnosis, adherence to Jones criteria, and secondary prophylaxis are essential to prevent long-term sequelae.
},
year = {2025}
}
TY - JOUR T1 - Rheumatic Chorea Without Cardiac Involvement in a 10-Year-Old Girl from a Remote Area: Diagnostic and Management Challenges AU - Violita Iwamony AU - Nyoman Gina Henny Kristianti Y1 - 2025/10/27 PY - 2025 N1 - https://doi.org/10.11648/j.ajp.20251104.12 DO - 10.11648/j.ajp.20251104.12 T2 - American Journal of Pediatrics JF - American Journal of Pediatrics JO - American Journal of Pediatrics SP - 201 EP - 206 PB - Science Publishing Group SN - 2472-0909 UR - https://doi.org/10.11648/j.ajp.20251104.12 AB - Rheumatic Chorea, also known as Sydenham Chorea, is a major neurological manifestation of acute rheumatic fever, an autoimmune complication following infection with Group A β-hemolytic streptococcus (GABHS). It remains common in low- and middle-income countries, where limited healthcare access may delay diagnosis and increase the risk of complications, particulary cardiac. We report a case of a 10-year-old girl from a remote area who presented with involuntary movements, joint pain, and a history of throat infection one month prior to symptom onset. Laboratory tests showed elevated erythrocyte sedimentation rate (ESR) and a positive Anti-streptolysin O (ASO) titer, indicating a recent streptococcal infection. Cardiac examination, including the electrocardiography (ECG), revealed no abnormalities. However, echocardiography, the gold standard for detecting subclinical carditis, was not performed due to lack of available resources. The patient was treated with haloperidol and trihexyphenidyl for chorea, penicillin G benzathine for eradication and prophylaxis of streotococcal infection, and aspirin for its anti-inflammatory effects. Clinical improvement was noted within one month of therapy. This case met the 2015 revised Jones criteria for moderate-risk populations, with major criteria including Sydenham chorea and polyarthralgia, and evidence of recent streptococcal infection (positive ASO). Absence of cardiac involvement may reflect early recognition and treatment, although echocardiography is required to exclude subclinical carditis. Symptomatic therapy and long-term antibiotic prophylaxis are crucial for preventing complications. Rheumatic Chorea can occur without cardiac involvement. Particularly in resource-limited remote areas, early diagnosis, adherence to Jones criteria, and secondary prophylaxis are essential to prevent long-term sequelae. VL - 11 IS - 4 ER -
Department of General Practitioner, Maren Hi Noho Renuat Hospital of Tual City, Maluku, Indonesia
Department of Paediatrics, Maren Hi Noho Renuat Hospital of Tual City, Maluku, Indonesia